A Chinese bus driver has died after a flying piece of metal smashed through his windscreen. He managed to put the brakes on, saving his passengers.
Category
News & Politics


What’s missing in how to improve police-community relations?
Written on 5/27/2015
It’s amazing that no federal, state or municipal political leader; no police administrator; and certainly no media talking head has come forward to ask why only ONE side of the narrative of how police-community relationships should change.
The clear theme that is evident in ALL of these police-involved citizen deaths is that a history of bad life choices made by citizens creates a confluence of circumstances resulting in unintended consequences that unfortunately have led to the deaths of those portrayed in the media and by uninformed activists as “innocents.”
Bad parenting, no parenting, the irresponsibility of young males to impregnate young naive females and then abandon their parental responsibilities; failing to embrace the benefits of education; failure to develop meaningful job skills; drugs abuse; gang involvement; embracing and glorifying gangsta rappers who forward a destructive narrative of drugs, crime, and disrespect/violence against police.
Nearly every so-called “victim” of these recent police-involved deaths had a history of criminal arrests; were fleeing from detention and arrest on foot and/or in vehicles; had verbally and physically resisted detention or arrest; had assaulted police with weapons; were in possession of weapons; and/or were under the influence of drugs during the encounter and altercations.
Where is the public’s ownership of these poor life decisions? Why aren’t the parents, the political leaders, the community activists, the media talking heads, celebrities, nationally prominent athletes and the jet setting, race bating civil rights “activists” such as Jesse Jackson and Al Sharpton extolling our children and citizens NOT to make these very obvious and poor life choices?
Why do some communities seem to have an overwhelming number of violent crimes, high levels of gang violence and drug abuse and interactions with police – and others either very low or almost no such instances? And why aren’t the obvious differences in these communities discussed?
Why are the false narratives such as “Hands up. Don’t shoot.” forwarded by the media, street activists, and our political leaders? Why are some segments of American society more intent upon assigning blame to the police; rather than accepting responsibility for their poor life choices?
The police are not psychologists, sociologists, criminologists and mental health practitioners. They are “First Responders.” Police respond to society’s problems; they can’t fix them. Police officers come from our communities; not from distant planets. They are us and we are them. Police get the training that YOU provide them with. Can they be better trained? Of course. Do they want and ask for better training and equipment? All the time, but YOU don’t want to pay for it. Do police need to be smart and better educated? Of course, but the problem is that agencies can’t find qualified officers because many who apply lack even the most basic education and personal skills to pass the tests to become a police officer. How are these issues the fault of police? Yet the public, politicians and the media consistently heap criticism on them.
If you want a dramatic national change in police-community relations, begin by first looking into the mirror as citizens and as a society and ask yourselves what are YOU willing to do to bring about this needed change? When will YOU begin accepting responsibility for YOUR actions? When you take this first step, you begin the journey upon the road towards positive change between yourselves and your police.
Dr. Ron Martinelli is a nationally renowned forensic criminologist and police expert with a national presence who investigates and independently reviews high-profile police-involved death cases at: martinelliandassociates.com
Written on 5/27/2015
It’s amazing that no federal, state or municipal political leader; no police administrator; and certainly no media talking head has come forward to ask why only ONE side of the narrative of how police-community relationships should change.
The clear theme that is evident in ALL of these police-involved citizen deaths is that a history of bad life choices made by citizens creates a confluence of circumstances resulting in unintended consequences that unfortunately have led to the deaths of those portrayed in the media and by uninformed activists as “innocents.”
Bad parenting, no parenting, the irresponsibility of young males to impregnate young naive females and then abandon their parental responsibilities; failing to embrace the benefits of education; failure to develop meaningful job skills; drugs abuse; gang involvement; embracing and glorifying gangsta rappers who forward a destructive narrative of drugs, crime, and disrespect/violence against police.
Nearly every so-called “victim”…
View original post 438 more words

 The Cognitive interview is derived from a range of sources of cognitive evidence relating mainly in the psychology of memory. It was formulated by combining a number of techniques to assist in allowing an interviewer, such as a police officer, to provide conditions that would allow for the greatest level of accuracy possible, in essence a systematic set of tools to allow access to someone’s memory without inadvertently altering it or not gaining the full insight due to poor phrasing. The Cognitive Interview (CI) is primarily used for witnesses and victims as it needs to assume a willing party. Suspects cannot be relied upon to tell the truth for obvious reasons, hence alternative approaches have been created for their interviewing, such as the controversial Reid Technique. The Cognitive Interview can also be used with children as witnesses, which is a significant advancement in police methods as to the historical
The Cognitive interview is derived from a range of sources of cognitive evidence relating mainly in the psychology of memory. It was formulated by combining a number of techniques to assist in allowing an interviewer, such as a police officer, to provide conditions that would allow for the greatest level of accuracy possible, in essence a systematic set of tools to allow access to someone’s memory without inadvertently altering it or not gaining the full insight due to poor phrasing. The Cognitive Interview (CI) is primarily used for witnesses and victims as it needs to assume a willing party. Suspects cannot be relied upon to tell the truth for obvious reasons, hence alternative approaches have been created for their interviewing, such as the controversial Reid Technique. The Cognitive Interview can also be used with children as witnesses, which is a significant advancement in police methods as to the historical
View original post 65 more words
Moving the Goalpost–Criminal Violations of HIPAA by PHS, Quest and USDTL
Information obtained under HIPAA Privacy Rule
1.August 6, 2014 to Langan with health materials 2. Quest-Clinical
The elements of a criminal offense under HIPAA are fairly straightforward. To commit a “criminal offense” under HIPAA, a person must knowingly and in violation of the HIPAA rules do one (or more) of the following three things.: use or cause to be used a unique health identifier, obtain individually identifiable health information relating to an individual or disclose individually identifiable health information to another person. Criminal penalties under HIPAA, tiered in accordance with the seriousness of the offense, range from a fine of up to $50,000 and/or imprisonment up to a year for a simple violation to a fine up to $100,000 and/or imprisonment up to five years for an offense committed under a false pretense and afine up to $250000 and/or imprisonment up to ten years for an offense committed with intent to sell, transfer, or use individually identifiable health information for commercial advantage , personal gain, or malicious harm.
One of the ways physician health programs are engaging in forensic fraud using laboratory developed tests (LDTs) is by changing them from “forensic” to “clinical” samples in order to bypass chain-of-custody. As there is no regulation or oversight of the entire testing process it is easy to do. PHPs have no oversight or regulation. Neither do the commercial drug testing labs using these tests. They are non-FDA approved and CLIA exempt so the only avenue of complaint is the College of American Pathologists (CAP) which is an accreditation agency that does not have the power to sanction.
In terms of criminal penalties I would aim for the $25000 and 10 year mark as the cumulative documentation of HIPAA breaches committed by PHS, Quest and USDTL under false pretense are many and severe.
The Department of Health and Human Services Office for Civil Rights confirmed that my blood test from July 1, 2011 was intentionally changed to a clinical specimen and sent to USDTL with specific instructions to process it as a clinical specimen. Under the updated HIPAA-Privacy Rule “patients’ have the right to request their records directly from labs without authorization of the ordering provider.
It is important to recognize that all three parties had misrepresented this test as “forensic” since 2011. I have been requesting the “external chain-of-custody” from Quest since December of 2011 and the “appended test” from V.P. of Laboratory Operations Joseph Jones since December of 2012 when I was informed that it was changed from positive to invalid on October 4, 2012.
The new documents provided by USDTL include the October 4, 2012 revised test contradicting Dr. Luis Sanchez letter that he “just found out about” the revised test 67-days later.
The importance of this cannot be overstated as I filed a complaint with the College of American Pathologists in January of 2012. The investigation confirmed my suspicion that the test was fraudulent and as a result CAP mandated that USDTL revise the test.
USDTL did so and reported it to Dr. Sanchez but both concealed it and Sanchez took action against my license the following week.
“Moving the Goalpost” is a frequent tactic of PHPs whereby they make a new allegation and disregard the original. By controlling the information that is provided they are able to suppress and conceal whatever they want by misusing existing health care confidentiality law.
The October 19, 2012 report for noncompliance with my contract was done under “color of law” and resulted in suspension of my medical license. The new documentation shows that all three parties were involved in the fraud and the coverup.
The information USDTL provided even contains an email from me to Joseph Jones from December of 2012 requesting that he provide a copy of the October 4, 2012 revision which he ignored.
In response to demand letters from my attorney all three defended themselves by claiming the July 1, 2011 test had absolutely nothing to do with my suspension and blamed it on my non-compliance. The new documentation shows that I was reported for noncompliance after Dr. Sanchez was made aware of the revised test.
As the three parties colluded to produce PHI and used it with malice in a conspiracy to commit fraud and I am therefore requesting that charges be filed against these parties under the HIPAA criminal statute:
The HIPAA criminal statute, 42 U.S.C.A. § 1320d-6, reads in pertinent part: ”A person who knowingly and in violation of this part— • uses or causes to be used a unique health identifier; • obtains individually identifiable health information relating to an individual; or discloses individual identifiable health information to another person, shall be punished as provided in subsection (b) of this section.” ”Whoever willfully causes an act to be done which if directly performed by him or another would be an offense against the United States, is punishable as a principal.” 18 U.S.C. § 2(b).
All three parties knew this was intentionally changed from a forensic to a clinical sample and PHI. Instead of correcting an error both Quest and USDTL took steps to conceal this information. In fact, the complicity of the three parties, cover-up and extent of damages caused by it make this the worst HIPAA-criminal violation to date. I can find nothing comparable and the damages have still not been corrected.
Luis Sanchez was notified of the invalidity of the test on October 4, 2012 but suppressed it for 67-days. This was a result of my complaint to the College of American Pathologists (CAP) that launched an investigation which revealed no external chain-of-custody existed for the specimen rendering it invalid. This was revealed to PHS on October 4th, 2012 but instead of disclosing this and correcting things Dr. Luis Sanchez reported me to the Board for “noncompliance” less than 2 weeks after it was revealed to him that the test was invalid. He then wrote a letter on December 11, 2012 stating that he “just found out” about the invalid test.
A Request to Inspect and Copy Protected Health Information and Authorization for Use or Disclosure of Patient’s Protected Health Information was sent to USDTL in July and August of 2014.
The July 1, 2011 PEth test was drawn as a forensic specimen and subsequently changed to “clinical” (rendering it PHI) at the request of Quest’s client, PHS, Inc on July 7th, 2011. USDTL sent the materials within the 30 day deadline.
Quest Diagnostics, however, refused to comply with my request for the authorization and release of information forms required for them to draw a clinical specimen (which I knew did not exist) as well as any documentation related to the request by PHS that Quest (in violation of all regulations, professional standards, and clinical laboratory law) changed a “forensic” to a “clinical” specimen. The Quest attorney insisted that I sign a “release” from PHS.
PHS and the colluding labs were apparently unaware of the updated HIPAA regulations removing the need to obtain a signed release from a “provider” to obtain PHI.
I only received it because the DOJ-OCR agreed that this was PHI and forced Quest to send it.
PHS manipulated the test, set up a system in which they could claim me non-compliant , then did so immediately after the test was amended and hoped I would never find out.
On 10/4/2012 USDTL amended the test noting “external chain of custody was not followed per standard protocol” invalidating the test (this was the result of the initial CAP investigation under the assumption it was a forensic test). This was faxed to PHS but they withheld this information from me and the Board of Registration in Medicine.
The very next week they deemed me “non-compliant.”
PHS then officially reported me to the BORM as “noncompliant” on 10/19/2012.
On 12/10/2012 I found out from Amy Daniels of CAP that the test had been amended. I then called PHS and they issued a letter the very next day 12/11/2012 stating “Yesterday, December 10, 2012 Physician Health Services (PHS) received a revision to a laboratory test” referring to the July 1, 2011 PEthstat. They then try to cover themselves by claiming they were not aware of any action taken by the board as a result of this test.
The documents reveal that PHS is violating multiple state and federal criminal laws including clinical laboratory laws. It not only involves forensic manipulation but sending laboratory specimens as “clinical” samples when they are not authorized to do so and misrepresenting them as “forensic.”
Joseph Jones goes on record as a strict advocate of quality control and chain-of-custody with his “Defense in Depth Strategy” video and multiple written documents proclaiming how USDTL follows strict and rigid protocol. Well the ” litigation packet” contradicts and even negates this. How can any of USDTLs testing be trusted in light of what is seen here.
There is nothing that correlates that test with me and for all intents and purposes it could be a positive template used specifically for this type of misconduct. They pointed out that it does not pass the common sense factor (i.e. what would an average person think under normal circumstances about this?)
What it shows is that Mary Howard of PHS changed a test that was drawn as a “forensic” test to “clinical.” She is listed as the ordering “physician.” None of the required information exists to obtain a clinical sample. There are no authorization forms signed by me or to whom the information can be disclosed–clear violations of “Prohibited Activities” under Massachusetts law governing clinical laboratories.
Quest and USDTL representation has already clarified that PHS requested this test be sent by Quest to USDTL as a “clinical sample” with specific instructions to process it as a “clinical” sample. PHS is a monitoring agency not a treatment provider.
A “clinical” laboratory specimen is defined (CLIA, DPH, HHS, state laboratory law, essentially everyone) by its use in the diagnosis and treatment of a patient in a doctor-patient relationship. It necessitates patient “care” which PHS is unable to legally provide as a “non-profit” charitable organization.
As this is both “bad-faith” and ultra vires “confidentiality agreements” and “peer review” protection should no longer be an issue. Just one removes it.
PHS is an agency that utilizes drug and alcohol screens to detect if doctors are using substances they are prohibited to use. It is not a clinical provider. I am sure Bresnahan has spun some sort of logical-fallacy argument to say it is, but the documentary facts negate this. Organizational purpose is clear. As a monitoring agency their drug and alcohol testing is forensic. This brings in to question their “charitable organization” non-profit status.
Accountability requires both the provision of information and justification for actions
Accountability also requires consequences for violations of professional standards-of-care, ethical codes of conduct and the law
PHS is able to do what they do by both blocking information and relying on others to overlook, table or otherwise dismiss valid complaints–complacent that these are good people helping doctors and protecting the public. The current incarnation does neither
There should be zero tolerance. PHS has been unaccountable for this type of behavior but this needs to be addressed.
Accountability requires both answerability, justification and consequences. There is no conceivable procedural, ethical or legal justification for what is shown here. The compounding of crimes over time is self-evident and therefore it is the responsibility of the state to hold him accountable for his crimes. The fact that he pontificates on professionalism and stands in judgment of others makes it even more important. There are no exceptions to the rules or the law..
And we now know why Quest was so reluctant to provide the records. Quest was complicit in this and obtained and processed a known forensic sample as “clinical” without any of the required documents. The test lists “ordering physician” as Mary Howard (who is a secretary at PHS). There are no signed release of information forms or authorization forms indicating who my PHI could be distributed to.
This is in violation of the HIPAA criminal statute. As a business associate It is my understanding PHS can be tied to it by the conspiracy statute.
There should be zero-tolerance for this type of criminal activity. There is no excuse for forensic manipulation and this must be addressed. The people who are engaging in this should be in jail yet they remain unscathed. This is a systemic problem that is best met with head on and in real time. It makes Annie Dookhan look like a girl scout.
7/1/2011—PHS requests blood test at Quest Diagnostics. No outside factors are involved in PHP requesting this. There is no outside complaint or concern behind it. I provide blood sample using my PHS unique identifier #1310
7/28/2011—verbal report that test was positive to the Board of Registration in medicine and requests I have a “reevaluation.”
I request test results in form of “litigation packet” but PHS tries to dissuade me and eventually threatens me with “unintended consequences.”
11/29/2011—PHS agrees to provide “litigation packet. Check dated 11/29/2011 is given for payment.
12/5/2011—Receive USDTL Litigation Packet Sole document from Quest is a fax that is time stamped and arrived 3 hours after the specimen was collected when I was in clinic at MGH rendering this impossible. In addition it is not my signature:
A fax from PHS to USDTL is also included requesting that my ID # 1310 and a “chain-of-custody” be added to an already positive specimen with no unique identifier connecting it to me.
A report dated 7/20/11 from USDTL “revised report per clients request” and “corrected donor ID from 46130 to 1310 and “corrected collection date to 7/1/2011”
Note this backdating of chain of custody and addition of my ID # is on 7/20/11 (one day after Dr. Luis Sanchez reported the test as positive to the Board of Registration in Medicine. )
Joseph Jones certifies that the specimen was processed with laboratory

Information obtained under HIPAA Privacy Rule
1.August 6, 2014 to Langan with health materials 2. Quest-Clinical

The elements of a criminal offense under HIPAA are fairly straightforward. To commit a “criminal offense” under HIPAA, a person must knowingly and in violation of the HIPAA rules do one (or more) of the following three things.: use or cause to be used a unique health identifier, obtain individually identifiable health information relating to an individual or disclose individually identifiable health information to another person. Criminal penalties under HIPAA, tiered in accordance with the seriousness of the offense, range from a fine of up to $50,000 and/or imprisonment up to a year for a simple violation to a fine up to $100,000 and/or imprisonment up to five years for an offense committed under a false pretense and a fine up to $250000 and/or imprisonment up to ten years for an…
View original post 3,279 more words
The following is part 1 in a series about death and dying in the medical context. This reflection was written by me earlier this year, before I sought out a Palliative Medicine elective. Part 2 will follow soon.
Until the last week of my sub-internship, I had never had a patient die on my watch. To be sure, I had patients on the cusp of dying – and some who did die, of course, when I was already on another rotation. I have been around dying patients who were on our team but were being taken care of by the other resident/medical student. But never a patient of my own, until my final year of medical school.
I have never been sure whether to consider myself lucky or unlucky. Is that a morbid way to think about it? That maybe I was lucky (and my patients were lucky) that they didn’t die on my watch? That maybe I was lucky that I hadn’t had to experience those awful and heartbreaking conversations with a patient’s family. In the Russian roulette game of hospital care and medical education, I felt spared.
At the same time – and I feel almost selfish for saying this – I considered myself unlucky. I had never been around a dying patient. I had never known what it meant to take care of someone in their final days. I had never had the opportunity to learn and grow as a person and a physician from those difficult moments.
My first clinical experience with death was during my sub-internship, with a woman with end-stage ovarian cancer. I had scrubbed in on her most recent debulking surgery, and I had followed her post-operatively. Though her overall prognosis was poor, she was progressing well after this most recent operation. Her pain and abdominal bloating were slightly improved. She was even about ready to go to a rehab facility; all the arrangements had been made for transfer.
But then she started failing – started not being able to get out of bed. Started being more confused about herself and her surroundings. Started sleeping more of the day. She was physically and mentally breaking down. The cancer burden was overwhelming her body, and she was not able to hold up.
This experience was undoubtedly sad, but the experience for me was compounded by the suddenness and relative unexpectedness of it all. “She was not dying when I met her!” I naively believed.
She did have terminal cancer, after all.
The emotional impact was heightened for me because of the fact that only one of her family members was with her until the end. I felt bad that nobody she knew from outside the hospital was there for; yet I hope our medical team was able to be a somewhat second family to her in her final days. I visited in on her, spoke with her relative, did everything non-medical I thought to try to make her comfortable (I didn’t know much).
When she passed, I imagined the briefest moment of stillness amongst the chaos, but the hospital quickly moved on. There was no closure, no reflection, almost no conversation. When the other team members who had helped take care of her found out the news, there was a general statement of sadness, but then it was back to work as usual. There was more work to be done, other patients to take care of.
I heard that the nursing and floor teams held a small commemoration for our patient later that week (as they do for any patient on the cancer floor who dies). I wasn’t aware it was happening, and I’m positive none of the medical team was present.
Do doctors not mourn, too? Don’t we all need a moment to breathe, to reflect on our relationship with that patient, and to acknowledge our emotions about their passing?
Why don’t they prepare us for this?
The following is part 1 in a series about death and dying in the medical context. This reflection was written by me earlier this year, before I sought out a Palliative Medicine elective. Part 2 will follow soon.

Until the last week of my sub-internship, I had never had a patient die on my watch. To be sure, I had patients on the cusp of dying – and some who did die, of course, when I was already on another rotation. I have been around dying patients who were on our team but were being taken care of by the other resident/medical student. But never a patient of my own, until my final year of medical school.
View original post 540 more words

Picture courtesy of: WKBN.com
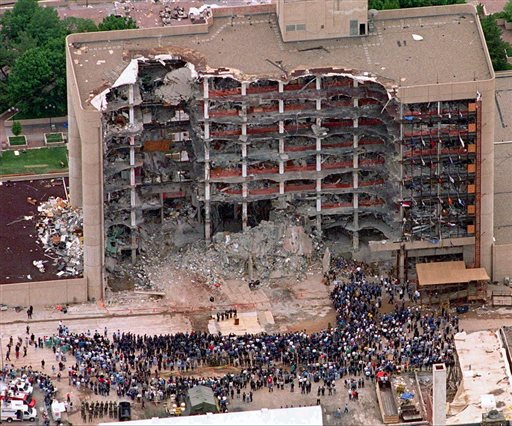
Oklahoma City Bombing 20th Anniversary on April 19th, 2015
In this May 5, 1995 file photo, a large group of search and rescue crew attends a memorial service in front of the Alfred P. Murrah Federal Building in Oklahoma City. The blast killed 168 people — including 19 children — injured hundreds more and caused hundreds of millions of dollars in damage to structures and vehicles.
Credit: Bill Waugh/AP file:

 Posted: 04/07/2015, 10:45am | Kim Janssen @ Chicago Sun Times
Posted: 04/07/2015, 10:45am | Kim Janssen @ Chicago Sun Times
A former Death Row inmate who was wrongfully convicted of a double murder after a Chicago cop withheld or fabricated evidence against him, then was left fuming when a federal jury awarded him just $80,000 in damages, is getting another chance to win the $18 million he says he deserves.

Bite mark evidence is very flawed and should only be used “in combination” with solid evidence when used in trial.
In otherwords, its not an exact science. A bite mark matching advocacy group just conducted a study that discredits bite mark evidence
Share on Facebook Share on Twitter Share on Google Plus Share via Email More Options
Resize Text Print Article Comments
By Radley Balko April 8
In February, I posted a four-part series on the forensic speciality of bite mark analysis. The series looked at the history of the field, how it came to be accepted by the courts as scientific evidence despite the lack of any real scientific research to support its basic assumptions, the innocent people who have been convicted based on bite mark analysis and how the bite mark matchers, advocacy groups like the American Board of Forensic Odontology and their supporters have waged aggressive, sometimes highly personal campaigns to undermine the credibility of people who have raised concerns about all of this.
The series ran during the annual American Academy of Forensic Sciences convention in Orlando, Florida. That conference included a presentation by Adam Freeman, who sits on the executive board of the ABFO, and Iain Pretty, who is not a member of the ABFO, has been critical of bite mark analysis and chairs the AAFS committee on forensic odontology.* Freeman and Pretty were to present the results of a study they had designed with David Senn, another ABFO member and a proponent of bite mark analysis.**
Senn in fact was the main witness for New York County Assistant District Attorney Melissa Mourges during a 2013 evidentiary hearing on the scientific validity of bite mark analysis in State v. Dean. That hearing was the first to assess the science behind bite mark matching since the field came under fire in a landmark 2009 report by the National Academy of Sciences. Ultimately, Senn and Mourges prevailed. Judge Maxwell Wiley ruled that the evidence could be admitted at Clarence Dean’s trial. In fact, to date, every court to rule on the admissibility of bite mark analysis has allowed it to be used as evidence. This, despite an ever increasing number of wrongful convictions, wrongful arrests, and lack of scientific research to support the field, and a new body of research suggesting that its core assumptions are false.
The study:
All of this makes the presentation by Pretty and Freeman particularly interesting. In response to mounting criticism, last year the ABFO released a “decision tree” for bite mark specialists to follow when performing their analysis. The “tree” is basically a flow chart. It begins by asking if there is sufficient evidence to know whether or not a suspicious mark is a human bite. It then asks whether it is in fact a bite, then what distinguish characteristics are noticeable in the bite, and so on.
But the problem with bite mark analysis was never the lack of a flow chart. The problem is that there has never been any real scientific research to support its two main underlying premises — that human dentition is unique, and that human skin is capable of registering and recording that uniqueness in a useful way. And the research that has been done strongly suggests those two premises are not true. The flow chart was just adding a series of procedures to a method of analysis that is entirely subjective, and that lacks basic scientific quantifiers like probability and margin for error.
Yet the ABFO wanted to show that its flow chart worked. So last year, the organization put together an exam to prove its effectiveness. Pretty and Freeman, with consultation from Senn and others within the organization, gave 39 ABFO-certified bite mark analysts photos of 100 bite marks, then asked them to answer three preliminary questions, all based on the decision tree chart. The average analyst who participated in the study had 20 years experience as a forensic odontologist. Here are the three questions they were asked:
Is there sufficient evidence in the presented materials to render an opinion on whether the patterned injury is a human bite mark?
Is it a human bite mark, not a human bite mark, or suggestive of a human bite mark?
Does the bite mark have distinct, identifiable arches and individual tooth marks?
That last question is asking if, once the analyst has determine that the mark is a human bite, the mark contains enough distinguishing features to be of value as evidence.
Interestingly, the intent of this study was to measure consensus, not whether the analysts were actually correct in their conclusions. Consensus is important, particularly in a field that relies so much on pattern matching and subjective analysis instead of quantifiable data. Consensus also shows predictability, which is also an important characteristic when assessing whether a field is legitimately based in science. There will of course occasionally be cases in which the evidence is ambiguous, but if a cross section of experts from a particular field consistently fail to reach consensus conclusions after looking at the same pieces of evidence, you have to start asking if the field is much more than guesswork.
But it’s also notable that there was no effort here to determine the rightness or wrongness of the answers. For example, if 10 out of 10 analysts agree that a mark on human skin is a human bite, that would suggest that the decision tree succeeded at fostering consensus. If only 7 out of 10 agree, that’s more troubling. But it would be even more troubling if the seven in the majority were also wrong.
The study didn’t measure for accuracy in part because the photos were taken from actual cases, so for many of them, whether or not the bite is actually human has never been definitively determined. But as I pointed out in my original series, it’s also keeping the field’s tendency to be more concerned about methodology than veracity. ABFO conducts its certification exams in a similar manner. The candidates are evaluated only on their method of analysis, not on on whether or not they’re actually correct in matching a bite mark to the correct dental mold.
This reflects an ugly reality about the pattern-matching fields of forensics: Because they’re so subjective, it isn’t difficult for attorneys on either side of a case to find an expert who will testify to the conclusion they’re looking for. In these fields then, the most important attribute in a witness is not that they be accurate, but that they sound accurate — that they be more convincing to a jury than the expert on the other side. Juries don’t like wishy-washy witnesses. They like witnesses who seem sure of themselves, who speak with authority. But in forensic specialties as subjective as pattern matching, certainty is a red flag. Most of the time, an honest witness should hedge, speak in probabilities, and avoid definitive conclusions. But this means that the least honest experts can often be the most persuasive, and there’s a clear incentive for prosecutors and defense attorneys to seek them out.
Finally, note that this study also did not ask the examinees to actually match a mark to the teeth of an individual human being the way this sort of evidence would be presented in court. (A previous competency test administered by bite mark critic Michael Bowers in 1999 found a 60 percent error rate among the analyst test takers.) It only asked the three preliminary questions above.
So in sum, this study only measured the ability of ABFO-certified experts to come to a consensus, and only on the most basic, preliminary questions about a piece of evidence.
The results
Even within these limited parameters, and even when designed and administered by the field’s biggest advocates, this study shows that bite mark analysis fails.
The first question — again, whether the test provided sufficient evidence to determine whether or not the photographed mark was a human bite — isthe most basic question a bite mark specialist should answer before performing an analysis. Yet the 39 analysts came to unanimous agreement on just 4 of the 100 case studies. In only 20 of the 100 was there agreement of 90 percent or more on this question. By the time the analysts finished question two — whether the photographed mark is indeed a human bite — there remained only 16 of 100 cases in which 90 percent or more of the analysts were still in agreement. And there were only 38 cases in which at least 75 percent were still in agreement. (These figure come from my own examination of the raw data, as well as processing of the data done by the Innocence Project.)
By the time the analysts finished question three, they were significantly fractionalized on nearly all the cases. Of the initial 100, there remained just 8 case studies in which at least 90 percent of the analysts were still in agreement.
“These results are really disturbing,” says Paul Giannelli, a law professor at Cast Western Reserve University who specializes in scientific evidence. Giannelli also serves on the National Commission on Forensic Science, started by President Obama to address and remedy the shortcomings in forensic evidence outlined in that 2009 NAS report. “But they aren’t all that surprising. There have been a number of cases over the years in which one bite mark analyst testified that a mark was a human mark, while another testified it was something entirely different, for example a bug bite, or an indentation from a belt buckle.”
Peter Bush, who with his wife Mary heads up the University of Buffalo research team that has cast doubt on the integrity of bite mark analysis (and who has been attacked by the community of bite mark analysts and their supporters for that research), agrees: “When there have been exonerations of people convicted with bite mark evidence, the forensic odontologists have said that the problem is with the analysts — that they’re rogue or incompetent experts who didn’t do the analysis properly. This is just another piece of evidence that’s it’s both of these things. It’s the improper analysis, but it’s also the very nature of the evidence itself.”
To put these results in perspective, it might help to ask what might have happened if a similar exam had been given to specialists from a more science-based field of forensics, such as DNA analysis.
“It would be difficult to set up a DNA test that was exactly the same, but if you could, you’d see overwhelming agreement,” Giannelli says. “I’d expect it to be unanimous. And on the questions where it wasn’t unanimous, you’d be able to go back and find the source of the problem — whether it was tainted evidence, or some glitch in the exam. With bite mark analysis, you can’t really even go back, because it’s just a subjective disagreement over what the analysts are seeing.”
Chris Fabricant, the director of strategic litigation for the Innocence Project who is challenging bite mark evidence in several cases across the country, points to a similar study of fingerprint analysts published in 2011 that found 99 percent agreement. “Contrast that to some of the questions in this study, in which the level of agreement among the analysts was only slightly better than randomness,” Fabricant says.
The reaction
The bite mark community reacted with shock, disappointment, and ultimately an effort to suppress the results of the study. According to reliable sources within the ABFO, David Senn initially wanted to cancel the panel at the AAFS conference in which Freeman and Pretty were to present the results. These sources say Senn was astonished at the results, and told other members of the ABFO that he was “reeling” from them. He also apologized to the organization for his role in the study.
In the end, the organization did proceed with the presentation of the results, but then played down their significance. Newly-elected ABFO president Gary Berman briefly mentioned the study in his quarterly message to the organization’s members.
In order to improve the study of bitemarks the ABFO developed a decision tree to assist practitioners in the proper selection and pathways of analysis in bitemark analysis. The ABFO has conducted preliminary research, presented in Orlando, designed to evaluate the first step of a revised decision tree; statistical analysis of the study showed inconsistent overall agreement among the individuals who participated in the project. The ABFO in reaffirming its commitment to ensure accuracy in bitemark analysis is revising the decision tree to ensure reliable results by forensic dentists and will be conducting additional studies this year.
While it’s commendable that the ABFO is attempting to create guidelines that will “ensure reliable results,” it’s far more troubling that the current guidelines don’t, that the unreliable results those guidelines produce have for years been used and continue to be used in court, and that rather than running to courtrooms across the country to halt the convictions, imprisonments and pending executions based on the results, the organization continues to fight for its members’ ability to testify using the very analysis it now concedes is flawed.
In an email in response to my query, Berman blamed the poor design of the study for the results. “Post analyses of the results indicate that the design of the survey and the design of Step 1 of the decision tree may be flawed, and that an ABFO guideline term may be the root cause,” Berman wrote. “The troublesome term, ‘suggestive of a human bitemark’, is one of the currently recommended terms for confidence that a pattern is or is not a bitemark.”
Berman writes that some of the test-takers may have answered the first question in the affirmative (that there was sufficient evidence to show that the mark was a human bite), but then changed their mind as they answered the other questions. He writes, “they were loathe to go back and change the answer to the negative . . . Instead they selected the hedged, and available third choice, ‘suggestive of a human bitemark.’”
Berman’s explanation raises another common criticism made by skeptics of bite mark evidence, although perhaps he raised it inadvertently: Because so much of their value as expert witnesses relies on their credibility, there’s a strong disincentive to change their minds about their conclusions once they’ve made them, even when new evidence suggests they should. If an analyst is loathe to admit a mistake in an anonymous proficiency study, it doesn’t bode well for his ability to admit to a mistake after putting his name and reputation behind court testimony, or in an affidavit leading to an arrest.
Indeed, bite mark analysts have concocted some fantastic theories of culpability even after a suspect convicted based on their testimony was found not to be a match to the semen taken from a victim who was raped, or even to the saliva taken from the bite mark itself. On more than one occasion, for example, a bite mark analyst has confronted a DNA mismatch on semen taken from a rape victim by arguing that someone else must have raped the victim while the suspect implicated by their testimony must have held the suspect down and bit her.
But even more concerning than the results of the study itself, the ABFO has since decided to hold off on publishing those results until the organization can tweak the design of the study and conduct it again, a process that’s expected to take at least a year.
“If this were truly a science-based organization, I would not only expect them to be extremely troubled by the results of this study, I would expect them to want to publish the results,” says Paul Giannelli. “And sooner rather than later, so that they could be considered in any pending criminal cases in which bite mark evidence is a factor.”
The ABFO did release the raw data from the study in spreadsheet form to a few people, but won’t release the presentation given at the AAFS meeting, nor will they publish the data in a journal or another publicly assessable format, at least until the completion of the second study. “We are in the process of modifying the decision tree, the language, and then we will be running the study again,” Adam Freeman wrote in response to an email query. “The results of both studies will then be sent to the [Journal of Forensic Sciences] for publication.The release of the presentation at this point would be premature. ”
Critics like Fabricant are skeptical. “If the results had been more to their liking, I can’t imagine that they’d be objecting over the language in their own study, then taking another year or so to rerun the study to get more favorable results before releasing the data. In the meantime, people are suffering in prison. Some are fighting a death sentence.”
One of the pending criminal cases is the one mentioned at the start of this post: that of Clarence Dean, which is expected to go to trial sometime this year. As noted above, that case included an important evidentiary hearing in which a New York judge ruled that bite mark evidence is admissible and scientifically valid. Many other judges have made that ruling in the past, but this was the first such ruling since the publication of the NAS report in 2009. The prosecutor in Dean’s case is Melissa Mourges, a fierce advocate for bite mark matching who, as I explained in the series in February, has not only advocated for bite mark analysis as a field, but has waged nasty, often highly personal attacks on those who have raised concerns about its legitimacy.
Mourges included a reproduction of the ABFO’s “decision tree” in her brief for the bite mark hearing in the Dean case. She cited the tree as another example of the bite mark community’s dedication to accuracy:
An important Guideline revision was added in February 2013 when the ABFO voted to include a bitemark flow chart or decision tree, included below. Properly used, the decision tree will guide forensic odontologists’ investigatory paths leading to proper conclusions based on the quality of the bitemark and the teeth of the suspected biters. This new guideline offers specific recommendations for forming degrees of linkage conclusions based on the quality of both injury features and suspected biter dentitions.
Mourges attended the presentation by Pretty and Freeman at the AAFS conference in February. I reached out to the Manhattan DA’s office where Mourges works to ask for her official reaction to the study. She didn’t respond, but the office did issue a statement from Chief Assistant District Attorney Karen Friedman Agnifilo:
This study reinforces the importance of basing decisions on the best possible evidence available. The use of forensic odontology, properly performed, has been and continues to be a valuable tool to aid in the identification of assailants and can also be used to help place victims, many of whom are children, out of harm’s way. Equally important, forensic odontology is used to exclude and exonerate suspects. Each time an injury is recognized as a bitemark and swabbed, investigators gain both DNA evidence and potential bitemark identification. Forensic odontology differs from DNA evidence in that it may not be dispositive, but it is probative. Undeniably, bitemarks have significant evidentiary value, which is why this type of evidence is admissible in all 50 states.
Agnifilo’s statement conflates a lot of issues, and I examined several of the points she makes in the February series. But briefly, few would object to swabbing potential bite marks for DNA. Rather, critics of bite mark evidence fault the attempt to match marks on human skin to human teeth. The fact that bite mark evidence is admissible in all 50 states is convincing only if you believe the courts have done an adequate job of keep bad science out of criminal cases. Part two of the February series argues that they haven’t. Agnifilo’s point about the quality of the evidence is a good one. But it remains true that even with the most pristine bite mark evidence, there’s no scientific research to support the contention that the marks we make with our teeth are individually, or to what extent they’re unique, or that, even if they were unique, that human skin is capable of preserving that uniqueness in a way that allows it to be analyzed.
The Manhattan DA’s office insistence on standing behind bite mark evidence is interesting in and of itself. Current Manhattan DA Cyrus Vance, Jr., was elected in 2009 on a platform of “community justice,” and won endorsements from criminal justice reform advocates — including, interestingly, Peter Neufeld and Barry Scheck, co-founders of the same Innocence Project that is now feuding with Mourges in court. On its website, Vance’s office stresses the importance of fairness and sound evidence in preventing wrongful convictions:
The Manhattan District Attorney’s Office spares no effort in seeking justice in every case that comes before it. Through the years and around the country, innocent men and women have been convicted of crimes they did not commit. This not only robs an innocent person of his or her freedom, it leaves a criminal on the street, free to commit more crimes.
To protect New Yorkers and ensure justice, District Attorney Vance created the Conviction Integrity Program in March 2010. The Program is comprehensive in scope, and is unique in purpose: not only does it address claims of actual innocence, it also seeks to prevent wrongful convictions from occurring . . .
The Conviction Integrity Policy Advisory Panel is comprised of leading criminal justice experts, including legal scholars and former prosecutors, who advise the Office on national best practices and evolving issues in the area of wrongful convictions.
The work of the Conviction Integrity Program, combined with the Office’s commitment to using the most advanced scientific and investigative tools available, has made the cases brought by the Office stronger for victims and more fair for defendants.
But meanwhile, at least two of Vance’s top lieutenants continue to defend a field of forensics that has contributed to at least 24 wrongful convictions and arrests around the country, despite numerous studies showing it lacks any basis in science, including one organized by the field’s leading advocacy organization.
Finally, I noted in my original series that last fall, the National Institute for Science and Technology announced the members of the forensic odontology subcommittee that will study the scientific validity of bite mark matching. The committee is one of several that will study various fields of forensics as part of the federal government’s push toward reform in light of the 2009 NAS report. Incredibly, 10 of the 16 members are either practicing bite mark analysts, or are open advocates of the practice, including the chairman, Robert Barsley. It’s a development one critic of bite mark matching likened to starting a committee to investigate the scientific validity of astrology, then stacking it with astrologists.
Pretty and Freeman’s study is a major development in the field of bite mark analysis. It’s one you’d think would attract the attention of the committee charged with investigating whether bite mark analysis is suitable for court. The committee held its first meeting on February 16. The results of the ABFO study were by then well known to the members affiliated with ABFO. According to the webcast and public notes from the meeting, chairman Barsley did include the ABFO “decision tree” in his presentation. He also incorrectly compared the uniqueness of bite marks to fingerprints, and noted that while he couldn’t point to a citation of a study showing that human dentition is unique, “there are studies that lead us to believe this is true.” (In fact, the only peer-reviewed, scientifically rigorous study of the uniqueness of human dentition has been conducted by Peter and Mary Bush’s team, and they’ve found no basis for that assertion.) Curiously missing from Barsley’s presentation was any discussion of the ABFO study showing that the decision tree failed to produce a consensus among even the ABFO’s most experienced analysts.
As the ABFO hems and haws on this study and takes another year to redesign it, ostensibly to achieve more favorable results, bite mark evidence continues to be used in criminal cases, and existing bite mark cases continue to move forward. Over the last several months there have been new filings in the death penalty cases of Eddie Lee Howard in Mississippi, and Jimmie Duncan in Louisiana. At least 15 people convicted with bite mark evidence are currently awaiting execution.
Meanwhile, just last week a sheriff in northern Indiana announced that he’ll be assembling a “forensic dentistry team” within his department. From the Chicago Tribune:
Sheriff David Reynolds recently swore in three local dentists as part of the department’s forensic dentistry team . . .
The dentists will do everything from matching bite marks with suspects or victims, to using dental records to identify victim’s remains, Reynolds said . . .
Over the years, Reynolds has used forensic dentists a number of ways.
“We used them for rape cases, investigating bite marks,” he said, as well as for remains . . .
“There were other cases where people were bitten and we were able to take (dental) models and pictures and match them up to bite marks on the victims.”
So even as we await the results of the ABFO’s do-over on its own study to assess the validity of this field, not only do those convicted due to bite mark analysis remain in prison, law enforcement groups are still using it to win convictions. It’s almost as if those 24 exonerations never happened.
(*Forensic odontology or forensic dentistry, includes the controversial field of bite mark matching, but also the more accepted practice of using dental records to identify human remains.)
(**Senn did not respond to my request for comment. In an email, Pretty acknowledged the study, the results, and that the ABFO will be conducting another study to be published next year. But because the study was administered by the ABFO, using ABFO case studies, he wrote that “it would be wrong of me to make any comments on the work beyond those that were made at the AAFS.”)
Radley Balko blogs about criminal justice, the drug war and civil liberties for The Washington Post. He is the author of the book “Rise of the Warrior Cop: The Militarization of America’s Police Forces.”
Share on Facebook
Share on Twitter
Comments
Most Read
1
Think Walter Scott’s death is ‘another Ferguson’? Cops don’t.
2
Apple’s new diverse emoji are even more problematic than before
3
Enough with the Scandinavians already
4
The Insiders: The Democratic Whackjob Survey
5
The sugar lobby’s sour tactics
The Most Popular All Over
Salon
Rand Paul just walked out of an interview after being pressed on a question
The Baltimore Sun
Commercial real estate boom reaches Baltimore
The Atlantic
The Abuse of Satire
The Most Popular stories around the web
Get the Opinions Newsletter
Free daily updates delivered just for you.
Our Online Games
Play right from this page
mahjongg-dimensions
Mahjongg Dimensions
Genre(s): Strategy
It’s 3D Mahjongg- you don’t even need to wear 3D glasses!
sudoku
Sudoku
Genre(s): Strategy
Put on your Sudoku hat and get ready for a challenging Sudoku puzzle!
daily-crossword
Daily Crossword
Genre(s): Word
Same fun of crosswords but online!
vegas-world
Vegas World
Genre(s): Card
Vegas World brings synchronous multiplayer gameplay to all of its casino-based classics.
washingtonpost.com
© 1996-2015 The Washington Post
Help and Contact Us
Terms of Service
Privacy Policy
Submissions and Discussion Policy
RSS Terms of Service
Ad Choices


The FBI’s new South Florida field office in Miramar. (Source: CBS4)
MIAMI (CBSMiami) – There will be a ribbon cutting and dedication ceremony Friday for the FBI’s new South Florida field office in Miramar.
FBI Director James Comey and U.S. Rep. Frederica Wilson are scheduled to officially open the building which is named for agents Benjamin P. Grogan and Jerry L. Dove, who were killed in a gun battle with bank robbers in South Miami-Dade on Friday, April 11, 1986. The firefight is still considered the bloodiest in the history of the FBI. Agent Grogan was a 25 year veteran of the Bureau. Agent Dove had been with the FBI for four years.
“The naming ceremony and dedication is a fitting tribute to Special Agents Benjamin P. Grogan and Jerry L. Dove. These brave men answered the call of duty and gave their lives to keep our streets, communities and country safe. We owe them and their families a debt of gratitude that can never be repaid,” said Wilson in a statement.
The new $194 million office building contains 330,000 square feet and sits on a 20-acre site adjacent to In terstate 75.
terstate 75.
For 28 years, the FBI’s South Florida headquarters was located in North Miami Beach. The field office has jurisdiction over federal cases along Florida’s southeast coast from Vero Beach to Key West.
(TM and © Copyright 2015 CBS Radio Inc. and its relevant subsidiaries. CBS RADIO and EYE Logo TM and Copyright 2015 CBS Broadcasting Inc. Used under license. All Rights Reserved. This material may not be published, broadcast, rewritten, or redistributed. The Associated Press contributed to this report.)
….. In 5 minutes.")
How I Finally Understood my 401(k)….. In 5 minutes.

4 Surgeries to Avoid via: AARP


WE RECOMMEND

It has been several days since hundreds of letters from the Santa Barbara County health Department were mailed to patients of a local clinic. Those letters warn patients to get tested for Hepatitis B, C, and HIV. 
“It’s the accident that just keeps on giving,” says Teresa Turner, a resident of Atascadero.
In 2011, 55-year old Turner says a drunk driver crashed into her, sending her to Dr. Allen Thomashefsky’s Santa Barbara Medical Clinic.
“Dr. Thomashefsky is a very friendly person, he seems to be a good guy,” says Turner. “The office was very clean and there was nothing out of the ordinary.”
At his office, Turner says she underwent therapy.
“Neck, back, and abdominal muscle,” says Turner. “I had several injections.”
When say this week’s news, a familiar face came up.
“It was announcing who the doctor was and it was Dr. Thomashefsky,” says Turner.
A phone call later to the Santa Barbara County Health Department, Turner was told she needs to get tested for possible Hepatitis B, C, and HIV. An appointment that could not come soon enough.
“Monday although it is only a couple of days away, it seems like it is very far away,” says Turner. “They are infectious diseases and I am concerned that they could have been shared with someone else.”
Turner says she knows the test results could be life changing.
“If I was to be infected by one of those, you feel like you are kind of labeled with a virus, how are people going to treat you,” says Turner.
She has made an appointment with her doctor in Paso Robles and hopes her story will help others take the necessary steps to move on.
“Because you don’t want to hide from this,” says Turner. “It is a very important and serious issue and you have to go on that path and deal with it.”
Atascadero woman finds out she could be exposed to HIV, Hepatiti.




















